


Podcast: Play in new window | Download
Hi it’s Patrik Hutzel from INTENSIVE CARE AT HOME where we provide tailor made solutions for long-term ventilated Adults & Children with Tracheostomies and where we also provide tailor made solutions for hospitals and Intensive Care Units whilst providing quality services for long-term ventilated patients and medically complex patients at home, including home TPN.
In last week’s blog, I talked about,
IS THE NDIS NEGLECTING AND KILLING VENTILATED AND TRACHEOSTOMY CLIENTS IN THE COMMUNITY? (PART 2)
You can check out last week’s blog by clicking on the link below this video:
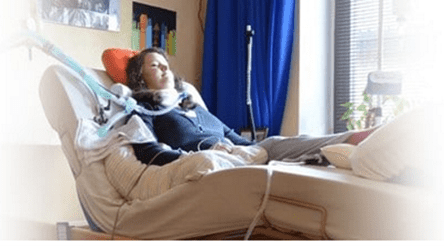
Trying to Get Intensive Care at Home with Ventilation & Tracheostomy & Dialysis Care for My Mother
Good morning, good evening, good afternoon, wherever you are. Welcome to another Intensive Care at Home and Intensive Care Hotline. To begin with, start typing in the numbers you can dial in live on the show here, if you like. I’ll just type in the numbers and then we can get started. If you want to dial in live on the show with your questions, please, you can dial in or type your questions into the chat pad. Let’s get started.
Today’s topic for Intensive Care at Home and Intensive Care Hotline is, “Trying to get Intensive Care at Home with ventilation, tracheostomy, and dialysis for my mom.” It’s a question we get all the time and I want to highlight today how you can get that for your mom and get her home.
Now, before I go more into today’s topic, I quickly want to talk about what makes me qualified to talk about these topics, anything intensive care related and Intensive Care at Home related. My name is Patrik Hutzel. I’m a critical care nurse by background. I have been working in intensive care/critical care for over 20 years in three different countries. I am the founder of intensivecareathome.com, where we are providing intensive home care nursing for predominantly long-term ventilated adults and children with tracheostomies and otherwise medically complex patients that are in need of intensive care nurses at home. During my time in intensive care, I have also worked as a nurse unit manager for over five years. I can talk about intensive care all day long. I can talk about Intensive Care at Home all day long. I’m also the founder of intensivecarehotline.com where we provide a consulting and advocacy service for families in intensive care. We help families in intensive care all around the world.
With Intensive Care at Home, before I answer today’s question, we are currently operating in Australia in all major capital cities where we have a number of highly skilled, intensive care nurses working with our clients at home. We employ hundreds of years of intensive care nursing experience and as far as I’m aware, we are the only company in the English-speaking world that has that area of expertise in the community and there is no other organization, as far as I’m aware, that has achieved third party accreditation for Intensive Care at Home. We are in the position to take patients home from intensive care directly. So, that’s a little bit about what gets me to this point to do this broadcast today, to do this live show.
Bit of housekeeping, you can type your questions into the chat pad, or you can dial in the show. I’ve typed the numbers in the chat pad here. You can dial me directly and you get me on the phone right here and there, and you can get on the show and get your questions answered here.
Let’s get started with today’s topic, “Trying to get Intensive Care at Home for my mom with ventilation, tracheostomy, and dialysis” and we had an email from a reader who was writing us in with her situation with her mom in ICU and she’s been in ICU for three months. She can’t come off the ventilator. She’s got dialysis needs and can she take her mother home? The short answer is yes, of course, this is something we’re absolutely capable of providing to our client.
How is it going to be set up? Well, similar to an intensive care bed, we are sending the intensive care nurses to your home and provide a 24-hour roster, so that your mom finally can leave ICU because you’re saying in your email that she doesn’t have any quality of life. She’s depressed and she can’t wean off the ventilator.
How can this be funded? For example, if you’re here in Australia, most of the clients are funded through the NDIS through the National Disability Insurance Scheme. If you are looking after funding in particular, you should contact us, of course, and then we can map out the next steps for you and with you how to get on the NDIS scheme.
But in some situations, you might have other funding sources available such as maybe the Department of Veteran Affairs, maybe it’s through an accident, then you might have an accident scheme stepping in. It really depends a little bit on where you’re coming from in terms of what led you to this situation. Sometimes it’s hospitals that are happy to fund because again, what we are providing is a win-win situation. You want your mom home, your mom wants to be at home, of course, the hospital wants a free bed. So, the hospital might have an interest in paying for it. Department of Health might have an interest in paying for it. Private health funds, of course, have an interest in paying for it because again, we are cutting the cost of an intensive care by around 50%. Again, it’s all about providing that win-win situation for everyone.
But in terms of your mother, how can she go home efficiently once the funding is there? We start hiring ICU nurses or depending on your location, we send you some of our nurses that are on our books already and especially when we take clients home for the first time, we have some of our senior nurses leading that because we’ve done many transitions home and you need the specialists to make that happen. It’s simple, but it’s not easy.
What do I mean by that? Of course, we need to focus on getting the right team for you and for your family. You want nurses coming to your home that are enthusiastic, that want to work with you, that live and breathe our vision and mission, which is to keep patients out of intensive care, and it needs to be the right fit for you and your family.
Then, how we go from there is we’ve got to organize the right equipment. We’ve got to organize ventilators, spare tracheostomies, tracheostomy dilator, resuscitation bag, equipment for the PEG (Percutaneous Endoscopic Gastrostomy), equipment for the dialysis, of course, spare ventilator, spare suction machine, monitoring all the documentation that needs to go in there. You probably need a hospital bed. You probably need a hoist to begin with until you can have a ceiling hoist or a lifting machine. There’s a number of things that need to get ready, but that’s all something that can be organized from our end.
Then, we also need to look at who’s the overseeing medical body or where’s the medical governance coming from? Sometimes it’s coming from the hospital. Sometimes it might even come from your GP. It can come from a respiratory doctor, so there’s a number of avenues again that we can show you and we can point you towards so that we can set it up properly.
That also leads me, “What are the goals?” You need to show us what are your mom’s goals? What does she want at home? She probably wants to spend time with family. I guess the major goal for now, the short-term goal is to get out of ICU as quickly as possible. That is the major goal. Then, once your mom is at home, then we can look at things like what does she want to do on a day-by-day basis? Where does she want to spend her time? Does she want to spend her time only at home? Are there avenues for her to go out? Most of our clients go out during the day, so this is contrasting an ICU bed where people think, “Well, that person won’t have any quality of life with what’s possible at home.” People live their lives, they’re very busy living their lives. They’re going out. They have friends, families coming over, which is very limited in ICU. Real improvement in quality of life. Some instances, quality of end of life, but where do people want to be and what needs to happen to make it happen? That’s what we are here to do really.
Then, once your mom is at home, once we’ve got a stable team, when we hire nurses for you, we usually go through staff introductions. We try to set up meet and greets with you and your family to make sure we’ve got the right fit for you. We try and introduce the staff, do some shadow shifts or some introduction shifts once we’ve got a few staff there. We’ve all done it before, and we can do the same for you. I know it sounds reasonably simple and it is simple. We just got to really find the right stuff for you. We know what to do with equipment and then we just continue the intensive care in the home. It’s no big deal really to put that in place.
Other things that we can organize or that need to be organized in a situation like that is nutrition. Your mom’s got a PEG tube. We need to organize nutrition. Again, that can all be organized. Other things that need to be organized are things such as an OT, physiotherapy, but again, we can help you with our network with setting that up.
Also, when I say we are sending intensive care nurses in the home, they have the same quality than the nurses in intensive care with the difference, most of them have home care experience and there is a difference between an intensive care nurse that has only ever worked in ICU and intensive care nurse that has worked in ICU and in home care. It’s a much more sensitive environment in a home care because everything is really driven by the client and by the family.
Our intensive care nurses, we believe that we have employed, understand the difference between an ICU and home care environment where we need to be sensitive to your requirements, to your requests. How do you want care to look like? How do you want your days to look like? How do you want your nights to look like? How do you want to have the shift times? The devil is in the detail. When should we be doing the tracheostomy changes? Are they being done at home? Do they need to be dying in the hospital? We can do them at home, but there are some rare situations when you need to do the tracheostomy changes in a hospital. What else needs to happen? Does your mom need regular nebulizers? How often do we change the inner tubes or inner cannulas? Number of things that need to happen, but again, we have done it many times and we can adapt to your mom’s situation.
I know your mom obviously has been in ICU now for three months and I know she’s, for lack of a better term, desperate to go home. I can totally understand that after three months in ICU, she would be so fed up by the environment. No natural daylight. It’s noisy, 24 hours a day. That’s another thing. Once your mom is at home in a family environment, it’s so much quieter. It’s so much nicer. Patients in ICU often have a disturbed day and night rhythm because of the environment. Whereas at home, it’s important to get back into a natural day and night rhythm, really important.
If there are no other questions in regards to whether ventilation, tracheostomy, and dialysis is possible at home, if there are no other questions, then I want to move on and start answering some other questions that we had coming in this week. But in the meantime, if you have any other questions to today’s topic, just type them in or call in on the numbers that I’ve just sent there in the chat pad.
Let me just answer some other questions that came through this week. Questions that came in this week, “When someone is in a coma being fed with a feeding tube and the patient has a UTI (urinary tract infection) plus pneumonia, could the sugar in the feeding tube add to the infection? What about probiotics after having been on antibiotics for months? Could it help causing the UTI and pneumonia?” I’ll read that again, “When someone is in an induced coma being fed with a feeding tube and the patient has a UTI plus a pneumonia, could the sugar in a feeding tube add to the infection?” Look, it’s been shown that not feeding in ICU is to the detriment of a patient. You need to start feeding early in ICU because if you’re not, the gut flora gets out of their normal pH range, and it could cause gastric ulcers or could potentially cause a GI or a gastric bleed. Not feeding would be detrimental for the patient and it would be detrimental for the long-term outcome of a patient, for long-term outcome of your loved one.
The answer to the first part of the question is, you need to start feeding. Could the sugar in the feeding tube add to the infection? I kind of doubt it. If someone has a UTI and has a pneumonia, well, a UTI is often a result of having a catheter in, a foley catheter in the bladder. That’s not the only reason, but that can be a reason. It could also be a reason, being immunocompromised. There could be other reasons for a UTI. Hygienic reasons and there could be a number of reasons. A pneumonia is, generally speaking, caused by an airway infection, chest infection travelling all the way down into the lungs. Therefore, again, it’s unlikely that the sugar in the feeding tube will add on to the infection.
Second part of your question, “What about probiotics after having been on antibiotics for months? Couldn’t it help causing the UTI and pneumonia?” This is probably more of a question that you need to discuss with your dietitian. Your loved one in ICU must have a dietitian and this is probably a question that should be answered by the dietitian that your loved one is having in ICU. I hope that helps with that question.
The next question that we had this week was, “My son’s been in ICU in the induced coma since the 20th of November 2022. He has a tracheostomy in place. The doctor’s claim his blood gas levels are not allowing him to breathe on his own.” Then, the second part of the question is, “I’m praying my son comes off that ventilator’s injury was supposedly aspiration pneumonia. The pneumonia is gone, but the lung is scarred, has a blood clot now as per the doctor’s report. I’m so grateful that he survived to this point. Will he survive any further?” That is a good question to ask.
Let’s just start with the first question. He’s been in a coma since the 20th of November 2022. By me reading out this email, today is the 15th of January. That’s nearly two months. That’s a long time. If his blood gas levels are not allowing him to breathe on his own, then there is a significant respiratory issue, and you need to find out what it is. Is it a pneumonia? Is it sleep apnea? Is he asthmatic? Does he have COPD (chronic obstructive pulmonary disease) ? You need to find out what’s causing it. If it’s a pneumonia, for example, they probably need to find out is it a bacterial pneumonia? Is it a viral pneumonia? Is it a fungal pneumonia? Then, treat it accordingly.
Initially, he obviously had an aspiration pneumonia and if the lungs are scarred and he has a blood clot now, that is definitely an inhibitor to get him off the ventilator. If he’s got scar tissue in the lungs, like with any other scar, it’s irreversible and that’ll be very challenging for your son to come off the ventilator if it’s a scar tissue, also known as lung fibrosis. Now, you haven’t shared how old your son is, but one next step might be, he’s got scar tissue, it’ll be difficult to get off the ventilator. That probably brings me back to our first question today, “Is tracheostomy, ventilation, and dialysis possible at home?” I think that might be a question you want to ask in this situation too, whether your son might be a candidate for going home if he can’t be weaned off the ventilator with scar tissue.
You haven’t shared how old your son is, but another avenue for your son might be to have a lung transplant. It depends on his overall condition, how old he is? And it’s definitely a question you should be asking and maybe you haven’t even considered that as an option. You are also saying that he’s got a blood clot now. I’m not sure whether you are referring to a pulmonary embolus or what you’re referring to, would be good if you could write in about that. I hope that answers that question.
Then, the next question that we’ve had this week is from John and John said, “Being told that our family member is “staying the same”, no improvement on the ventilator, but cognitive mental status is improving, and the ICU palliative care team are pushing to consider medical intervention as well as turning off the ventilator.” This is something unfortunately we see all the time where things apparently are improving, but the ICU is pushing for end of life.
Now, if, John, your family member’s cognitive and mental status is improving in particular, then my recommendation is to look for getting to the point where your family member can make up their own mind what they want. Surely that if they wake up, they would say that they don’t want to die. I think you need to get to that point to get the palliative care team off your back and the ICU team off your back.
This week in particular, we’ve had so many situations with clients where ICU teams were quite frankly pushing for end of life, not in a nice way and we were able to recommend some treatment options. We were able to recommend and also advocate for our clients to keep going with life support on religious grounds, on cultural grounds. Not every culture or every religion is saying, “It’s okay in my religion to just stop life support.” In my religion, I believe that we should keep going until the very end and one has to respect that. The reality is that patients’ wishes need to be respected, families’ wishes need to be respected in the absence of an advanced care directive.
It always boggles me, and it still boggles me how quick that ICUs are to push for end of life. They need the beds, we know that, and they think that if the patient was to survive, that there’s “no quality of life.” Well, you’ve just heard me talk about Intensive Care at Home. There’s definitely quality of life at home with the right support structure, with the right mindset, with the right people. I am still shocked in how quickly ICUs are trying to withdraw life support in certain situations. But in your situation, John, you simply need to push back, and you need to say what you want for your family member.
As a side note here, this is for any of you watching this, if you have a loved one in intensive care, you should be making very clear from day one when you are coming into intensive care what you would like. I understand the challenge here. The challenge is no one’s sitting at home doing research and thinking, “Oh, what if my family member goes into ICU next week? What question should I be asking?” No one is sitting at home wondering that no one’s doing the research. When you are then confronted with a situation like when your loved one is going into ICU, you don’t know where to start. You have no idea what to expect. You have no idea that the machinery that is intensive care can be quite ruthless and if you’re not prepared for it, you almost stand no chance in getting what you want.
Unfortunately, you can’t just presume that the ICU will do whatever is necessary and whatever is really in your loved one’s best interest. You can’t just automatically assume that. What you must assume is that ICUs are running a business and you must assume that ICUs will try and manage budgets, will try and manage staff, beds, equipment, and so forth. That’s what you must assume. All the communication that’s coming from an intensive care team is really all around that. It’s about priorities and sometimes unfortunately, your loved one is not a priority.
Case in point, this week we were working with a family who had their 48-year-old dad/husband in ICU after cardiac arrest and supposedly hypoxic brain injury. Clearly, the gentleman was deteriorating, and his CO2 (carbon dioxide) was rising and the ICU did not change the ventilation settings to get CO2 down saying that it was “not in his best interest to survive.” I’m a big believer that every patient in ICU needs to be given a chance. If they do survive, then you need to look at other options again, such as Intensive Care at Home, for example. There’s a number of things that can be done.
And again, you need to think ahead, and you need to get someone on side who can ask all the right clinical questions who knows what’s to come next, who can manage intensive care teams because most families in ICU have no idea how to manage intensive care teams.
Coming back to this 48-year-old man, they didn’t change the ventilator settings to get his CO2 down. Then, he dropped his blood pressure and after the family put some pressure on, we told the family what treatment options are there and they did use those treatment options, then his situation improved. Including they did change the ventilator settings and they got his CO2 down just as we predicted, but you got to ask the right questions. You also have to keep in mind if intensive care teams are not using the right treatment approach, potentially that could be perceived as medical negligence. Then, you’ve got to draw your own conclusions.
But you also need to understand, John, coming back to your question, originally about 90% of intensive care patients survive, approximately 90% of intensive care patients survive. You got to ask that question, “Why should your family member be the one out of 10 not surviving?” The odds are in your loved one’s favor. That is really important for you to keep in mind.
Again, no one is talking about quality of life, that if your loved one is surviving, what does that quality of life look like? No one knows that, but that’s not for the intensive care team to decide. That’s for you to decide what is quality of life? What’s acceptable for you and your family? What’s acceptable for your loved one? I do not agree with that nihilistic outlook of many intensive care units where they say and make the judgement of, “Well, that person won’t have any quality of life anyway.” Who’s to say that? I hope that helps, John.
Then, let’s go to the next question that we have this week, “My fiancé is in ICU in a critically induced coma. It’s been almost 72 hours. I wasn’t home when his collapse occurred, but I was told he went into cardiac arrest. He’s 55 years old and he’s had two previous heart attacks in the past. Can he survive?” That’s a great question. Look, if he’s had two previous heart attacks and he’s now had another cardiac arrest, my first question is, “Well, why did he have another cardiac arrest? Did he have cardiac surgery after this arrest? Did he have cardiac surgery after the last two heart attacks? What happened? Did he go to the catheter lab for an angiogram? For an angioplasty? Did he have cardiac surgery? What’s the treatment this time round? Again, has he been to cath lab? Has he had an angiogram? An angioplasty? Does he need cardiac surgery? Has he been referred to a cardiac surgeon?” Those are questions that need to be asked in a situation like this, but it’s very basic information that you’re giving me here, Susan.
The reason I’m saying that is you’ve heard me say before, the biggest challenge for families in intensive care that they don’t know what they don’t know. They don’t know what to look for. They don’t know what questions to ask, they don’t know their rights, and they don’t know how to manage doctors and nurses in intensive care. That’s exactly the challenge that you are facing here. When we work with clients one on one, we really need to either talk to the doctors and nurses directly to answer very specific ICU related questions or we need to look at medical records. Ideally, we do both. Ideally, we do both.
With what you’re sharing with me here, Susan, it’s not even 2% of the information me and my team would need to know to give you answers. This is why intensive care is such a highly specialized area. I’m talking about intensive care here all day long, but that’s after over 20 years of experience. Your fiancé has only been in ICU for two days and you’re barely scratching the surface here, barely scratching the surface.
Other questions to ask, Susan, in a situation like that is have they done cooling therapy, which often happens after cardiac arrest? Has he sustained a brain injury from the cardiac arrest? How long did CPR (cardiopulmonary resuscitation) take? How long was the “downtime”? Was there loss of oxygen to the brain for more than three minutes? Those are questions to ask.
In terms of the heart condition, what’s his ejection fraction or the contractility of the heart? Is he potentially on a balloon pump? Is he on ECMO (Extracorporeal membrane oxygenation)? What are his blood results? What are his ventilator settings? What medication are they using for the induced coma? Is he on inotropes or vasopressors? You can see I’m just scratching the surface here, but you need to ask all those questions. Hope that helps, Susan.
Another question we have this week is, “My stepdad is currently in the ICU in the U.K. for lung surgery to remove huge stage 4 metastatic renal cell carcinoma. He’s 55. He was diagnosed in November 2021. Operation was under the 15th of December ’22 to remove the left kidney. When the doctors were in there, they discovered the cancer had engulfed in the kidney, which was larger than a rugby ball and they had to remove the spleen part of the pancreas, different doctors said half the main vein to the heart and some off the wall. When he came out of sedation, he was talking and doing well. Two days later, they were worried about fluid in the abdomen, which resulted in him being rushed back to theatre for a left hemicolectomy. At this point, he was very weak but only a little oxygen on pain relief and they introduced antibiotics. Three days on from what we were told, his pancreas was still leaking fluids and needed a scan. Then, they decided it was best for them to go in and wash out the wound and look further into things. They discovered the right side of his bowel perforated and they had to take some away there as well. Now, his gut sepsis and his remaining organs are starting to fail. The doctor wanted to stop support, but we said it has to be his choice, to which the doctor told my mother she doesn’t have a choice. They will decide what to do. It’s a medical decision. Today, they have his breathing struggling and putting back on a ventilator with the view of theatre tomorrow for a tracheostomy, so they can drain the fluid off his lungs because he’s not strong enough to cough it up. But his heart rate has gone up and his blood pressure has gone down. I think the ventilator might have damaged his voice box. From Wayne.”
Thanks, Wayne, for sending in your dad’s or stepdad’s situation. Now, if they are doing a tracheostomy and he is going to theatre for another surgery, then I think they’re doing all the right things. In some jurisdictions, the doctors are “allowed” to make medical decisions, but that shouldn’t stop you from challenging it and shouldn’t stop you from getting second opinions. But in this situation when you’re telling me they’re taking him back for surgery, they’re giving him a tracheostomy, there’s no indication for me that they’re giving up, but you certainly have to watch the rhetoric that’s coming from intensive care teams. Again, you have to be one step ahead of them and knowing what’s coming and anticipate that.
Now, with the sepsis and his remaining organs are failing, the trouble is he’s got some form of abdominal sepsis probably and that is certainly always a challenge when there’s multiple organ failure to turn this around. It can be turned around, but it’s often not a quick fix. Patients might stay in ICU for quite some time. They may have difficulties getting off the ventilator. Certainly, multiple abdominal surgeries and it sounds to me like it’s got drain in his tummy and so forth. That can be very difficult. You may have to brace yourself here for a prolonged ICU stay with an uncertain outcome.
“They also think that the ventilator might have damaged his voice box.” You’re probably right there that prolonged intubation or prolonged tracheostomy will paralyze the vocal cords, and that is certainly a challenge. It also depends with your stepdad’s stage 4 cancer, has the cancer spread? Are there other metastases somewhere? Because that’ll be another challenge. Have they considered chemotherapy?
Also, with the left hemicolectomy, they would’ve removed large parts of the bowels, which is also a big challenge. With the sepsis, they would need to treat what I believe is an abdominal sepsis with probably strong antibiotics. I wouldn’t be surprised if he ends up on a dialysis machine, at least in the short term like if he needs hemofiltration. But again, if they are doing a tracheostomy and they continue treating him, then I believe the doctor’s words and his actions do not match. As long as they keep treating him, that’s probably a good thing because that’s what you want. That’s what your stepdad wants. Then again, you need to think about, do you want to take him home? If he doesn’t come off the ventilator, if he struggles coming off the ventilator, do you want to take him home with a service like Intensive Care at Home?
You see, what all of those situations have in common. As much as I would like to give everyone a quick fix, unfortunately, there is no quick fix. There’s only a long-term approach. Long-term approach for you means you’ve got to do your research. You’ve got to anticipate what’s coming next. You’ve got to manage the team there. You’ve got to get someone on your team that can help you with anticipating the next steps and we can do that here. In Intensive Care Hotline and Intensive Care at Home, you’ve got all your bases covered. Next, let’s go to the next question. I hope that helps, Wayne.
This is from Brian. Brian says, “Thank you for your help and I apologize for not replying earlier, but we’ve had a very difficult time, especially over the last 10 days. Today’s the seventh day that my wife has been free from a ventilator. However, this was not a simple and straightforward process. Early on the 2nd of January, my wife on a ventilator on CPAP mode, this was then changed to a BIVENT level or a BIPAP (Bilevel Positive Airway Pressure) level. On the 5th of January, we had a call to advise that my wife was dying. CO2 was building up and the team had to hand pump to get sufficient oxygen into my wife as the ventilator would not go to the pressures needed. This, at the time, was apparently an unsustainable situation. The ICU consultant’s advice the only way forward was to let my wife pass away by switching off the ventilator. This was done and we waited and waited. She’s still here. The two primary senior respiratory consultants are baffled. Currently, she’s once again receiving saline oxygen and is being fed by a nasogastric tube. The situation’s very fragile. What do you think is happening?”
Well, I can tell you what I think is happening here, Brian. I remember talking to you a couple of weeks ago. There are two things happening here. The ICU team here is extremely negative. They were anticipating the worst-case scenario from their end if they kept treating your wife.
What’s the worst-case scenario for an intensive care unit? Worst case scenario for an intensive care unit is to have a long-term patient in there looking after someone long-term with an uncertain outcome. Your wife clearly fitted that picture from memory when I spoke to you on the phone a couple of weeks ago. Now, I know you’re in the U.K., Brian, and I know in the U.K. at the moment, what’s happening there is really terrible because we have a number of clients in the U.K., and we can see the push towards end of life in most ICUs where we work with clients. It’s terrible. I do believe that the NHS has lost all moral and ethical grounds for patients and families in ICU.
I’m well aware that there’s a lot of good things happening in ICU, but because with the work that I’m doing and we see a lot of negatives and we see that nihilistic approach from intensive care teams, again, saying it’s “in the best interest” of someone to die. Well, unless someone has said they want to die, it’s not in their best interest. Life is worth living, even if people are on a ventilator. Ask our clients at intensive care whether they want to be dead or they want to be alive. Well, they all want to be alive.
Now, coming back to your situation, Brian, though, it tells me once again that intensive care teams are very poor predictors of the future. Sometimes, we have clients approaching us in similar situations where they say, “Well, I see you saying we need to stop life support and then my wife, my husband, my child, my parent, whatever, is going to die.” I say, “Well, how do you know?” That’s what I would’ve said to you if you had contacted me there and then I would’ve said to you, “Well, how do they know that your dad is going to die?” Your wife, I’m sorry. How do they know? Do they have a crystal ball? Clearly not. This is all about positioning your wife in a negative way. Again, what if you would’ve pushed for Intensive Care at Home, for example? This would’ve never happened in the first place. You got to get informed, Brian, here and take matters in your own hands. Do the research, know what your options are. I would never agree to end of life unless the person wants to. We all want to live. Given that she’s still alive, again, their predictions were very poor.
Now, what happens if your wife is deteriorating? She probably needs to go back on a ventilator. She should have probably never been taken off a ventilator in the first place. If the ventilator was not getting the pressure that was needed, could she have benefited from ECMO? I don’t know. I don’t have all the information. It’s a little bit of speculation here from my end, but you should ask the question, what would’ve been other treatment options? You didn’t ask the question at the time, what are other treatment options? Maybe ECMO would’ve been one of them.
Again, it comes back that families in intensive care don’t know what they don’t know. They don’t know what to look for. They don’t know what questions to ask. They don’t know their rights, and they don’t know how to manage doctors and nurses in intensive care. That’s exactly what’s happening here, Brian. You got to read between the lines in ICU. Now, they’ve cut off your options for your wife to have advanced treatment. I’m sure you didn’t want that.
Again, this is hopefully also a warning for other families in intensive care that you need to think ahead. You can’t just give in, especially in the U.K. at the moment in ICU, that’s happening. A lot of patients die because ICUs are withdrawing treatment prematurely or even worse, they’re withholding treatment. Unless families work with us, they don’t even know that the NHS is withholding treatment because we can see what’s happening. Hope that helps, Brian.
Let’s answer one more question and then we’re going to wrap this up today. This is from Cocane. Cocane says, “Our dad went into hospital for an operation on a fractured thigh. The doctors were giving anesthesia and during surgery, he had a cardiac arrest because he had a thrombosis. They’re saying my dad had six cardiac arrests during that period. They always brought him back. Since then, he’s been on a ventilator. Doctor did an MRI on the very next day. The brain was looking normal, but there is no clinical improvement after day seven. They did again another MRI and they said there is now severe hypoxic ischemic brain injury and they’re saying that my dad will remain in a permanent vegetative state. But as time passes on day 15, my dad opened his eyes, no pupil movements yet, but he’s also now moving his leg. The doctors are saying, “You can withdraw life support as there is not any good hope for any further recovery.” Please help me and guide.” Sure.
Again, similar to the other situations that I’ve just mentioned now, you should not give up if you don’t feel like giving up. You should put yourself in your dad’s shoes and find out what he would want. If you think he would want it to continue, continue. If you think your dad wants not to continue, then you should probably look into that, but you shouldn’t make any rush decisions one way or another. One way that I always say is when families say, “Well, what decision should we be making?” It’s quite simple. You should be making decisions today that you don’t regret in a year’s time. That’s how you should make decisions. Imagine you’re making a decision today that you want to withdraw life support today. Would you regret that in a year’s time? Don’t think about tomorrow. Don’t think about the next day. Think about a year’s time because we have many families coming to us saying, “Oh, last year, I decided that it’s “right” to withdraw treatment on my dad. And now, I regret it because I think, did I kill my dad?” They’re having second thoughts, and you are in the very same shoes here.
Now, if you are saying that they’re saying your dad is in a vegetative state, well, if he’s already opening eyes and moving his legs, what are the next steps? Is it likely for him to go backwards? Is it likely for him to move forward? I don’t know. I don’t know, but you need to think about what’s possible.
Again, coming back to Intensive Care at Home, can you take him home with ICU nurses and replicate the ICU, but at home? Most likely. But what you’re sharing with me, I think that is an option. Assuming he’s medically stable. You haven’t shared anything. I think that that is your next step, looking at home care. It’s quite simple. Simple, but not easy. Again, to everyone that’s watching this, I have solutions, but I don’t have a quick fix. We have solutions, but no quick fix.
Again, I just want to remind you, you can type your questions into the chat pad, or you can dial in live on the show if you have any questions on the numbers that I put in the chat pad. If there are no other questions, then I want to slowly wrap this up.
Maybe we’ll just do one more. One more question that came in this week from Tracy. Tracy writes, “They’re trying to give my dad a tracheostomy and he has mechanical ventilation. He yawned yesterday, which is something he hasn’t done before and he moves when I’m there, his eyes and stuff, and hence when I start praying for him, he’s really trying to fight and get better. I don’t think another surgery is the way to go. As to me, he’s just tired, but he’s more active and awake as the days go by. Please, may I have some advice? They’re trying to wean him off the ventilator. Is this the right thing to do?”
I’ll just answer that part of the question because there’s more to come. Is it the right thing to wean him off the ventilator? Absolutely. If they can avoid the tracheostomy, they should. The goal should always be to wean someone off a ventilator and the breathing tube full stop. That should be the number one goal. There should be no talk about tracheostomy. Once they’ve done everything beyond the shadow of a doubt to try and wean your dad off the ventilator with a breathing tube and it’s not working for whatever reason, then you can look at a tracheostomy. Weaning him off the ventilator is the right step, 100% to avoid the tracheostomy.
Then, your question goes on. “They said they won’t do anything without our consent and there’s risks to still being on mechanical ventilation, but the risks to me sound better than getting another invasive surgery and being out under sedation again. He’s stable, but he’s had brain surgery and that takes some time to heal. They’re saying we should do it to get him into a rehabilitation. I just hope and don’t know if we should let risks scare us into getting this surgery.” That is from Tracy. Tracy, great question and thanks for writing in.
Again, if he can’t be weaned off the ventilator with a breathing tube, he absolutely should have a tracheostomy. The risk of him staying on a breathing tube is higher. If he can’t be weaned off the ventilator, then it is to get a tracheostomy because if he stays on a breathing tube, most of the time, he needs to be in an induced coma. The longer he’s in an induced coma, the more he’s got muscle wastage. He’s getting deconditioned. Once he’s got the tracheostomy, they can wake him up, hopefully mobilize him, hopefully start with more physical therapy. The risk of him staying in an induced coma and the breathing tube is much higher than doing a tracheostomy. Assuming he’s not waking up and he’s not ready to be taken off the breathing tube, the cutoff is about two weeks. You shouldn’t have someone on a breathing tube for more than two weeks before you’re doing a tracheostomy. I hope that helps, Tracy, answering that question.
Yes, tracheostomy is invasive surgery, absolutely, but keeping him on a breathing tube and in an induced coma is doing more damage than having them do a tracheostomy. Again, that’s assuming he can’t be weaned off the ventilator, and he can’t be weaned off the breathing tube.
Another thing that you need to consider is with the brain surgery, you haven’t shared whether your dad is awake or whether he’s not awake. The more awake he is, the higher chances he can get off the ventilator. The more asleep he is, chances are lowering of him getting off the ventilator at least quickly. Then, a tracheostomy would probably be the right next step. I hope that helps, Tracy.
I want to wrap this up today, unless there are any other questions. Type your questions into the chat pad or you can call me directly on one of the numbers that I typed into the chat pad.
If there are no further questions, I would really appreciate if you give this video a like, give it a thumbs up. I would appreciate if you subscribed to my YouTube channel, for regular updates for families in intensive care. I would appreciate if you clicked the notification bell and share the video with your friends and families who have family members in intensive care to get the help they need.
Furthermore, if you have a loved one in intensive care, go to intensivecareathome.com, especially if you are looking for home care, go to intensivecareathome.com. We can help you with home care for your loved one with tracheostomy and ventilation, also with BIPAP or non-invasive ventilation, CPAP (Continuous positive airway pressure). We do home TPN. We do any clients at home that are in need of an intensive care nurse. We even have clients that are sometimes not in the ventilator, but they have other very complex clinical conditions, and they would be in intensive care otherwise, so we can help you with that.
If you need consulting and advocacy in intensive care, if you need questions answered for intensive care related subjects when you have a loved one in intensive care, go to intensivecarehotline.com. Call us on one of the numbers on the top of our website or simply email us to [email protected].
Please also check out our membership for families in intensive care at intensivecaresupport.org. There, you have access to me and my team, 24 hours a day, in a membership area and via email and we answer all questions, intensive care and Intensive Care at Home related.
We also offer medical record review, for our clients in intensive care. We do medical record reviews while your loved one is in intensive care and also after intensive care, especially if you are concerned about medical negligence, but it’s so much better if we can review them in real time because in real time, we can give you real time feedback and we can ask the right questions to the doctors and the nurses in real time.
That’s it for today.
I’ll do another live stream next week, again, 10:30 AM Sydney, Melbourne time. That is 6:30 PM Eastern Standard Time on a Saturday night, which is 3:30 PM Pacific Time. I’m looking forward to catch you here.
Have a look at the quick tip videos that are published during the week. I’m looking forward to engaging with you again.
Again, if you need Intensive Care at Home, have a look at the intensivecareathome.com and contact us through the website or call us on one of the numbers on the top of our website.
Take care for now. I appreciate your support.
Take care.
Now, if you have a loved one in intensive care and you want to go home with our service intensive care at home and if you want to find out how to get funding for our service and how it all works, please contact us on one of the numbers on the top of our website, or send me an email to [email protected]. That’s Patrik, just with a K at the end.
Please also have a look at our case studies because there we highlight more about what we can do for clients, how clients can live at home with ventilation and tracheostomies and you can look at our case studies as well at our service section.
Intensive care at home Case studies
And if you are at home already and you need support for your critically ill loved one at home, and you have insufficient support or insufficient funding, please contact us as well. We can help you with all of that.
And if you are an intensive care nurse or a pediatric intensive care nurse with a minimum of two years, ICU or pediatric ICU experience, and you ideally have a critical care certificate, please contact us as well. Check out our career section on our website. We are currently hiring ICU and pediatric ICU nurses for clients in the Melbourne metropolitan area, Northern suburbs, Sunbury, Bendigo, Mornington Peninsula, Bittern, Patterson Lakes, Frankston area, South Gippsland, Drouin, Warragul, Trida, Trafalgar and Moe as well as Wollongong in New South Wales.
www.intensivecareathome.com/careers
So we are also an NDIS (National Disability Insurance Scheme), TAC (Victoria) and DVA (Department of Veteran affairs) approved community service provider in Australia. Also have a look at our range of full service provisions.
Thank you for watching this video and thank you for tuning into this week’s blog.
This is Patrik from Intensive Care at Home and I’ll see you again next week in another update.
RELATED LINKS:
 Helping hospitals and Intensive Care Units in particular, freeing up beds and staff
Transitioning long-term ventilated Adults& Children out of Intensive Care- making it happen with the latest guidelines
The 5 things you didn’t know INTENSIVE CARE AT HOME can do for your ICU
5 SERIOUS PROBLEMS AND FRUSTRATIONS THAT ARE NOT ADDRESSED FOR LONG-TERM VENTILATED ADULTS& CHILDREN WITH TRACHEOSTOMIES IN INTENSIVE CARE!
What are indications for mechanical home ventilation and Intensive Care At Home?
Helping hospitals and Intensive Care Units in particular, freeing up beds and staff
Transitioning long-term ventilated Adults& Children out of Intensive Care- making it happen with the latest guidelines
The 5 things you didn’t know INTENSIVE CARE AT HOME can do for your ICU
5 SERIOUS PROBLEMS AND FRUSTRATIONS THAT ARE NOT ADDRESSED FOR LONG-TERM VENTILATED ADULTS& CHILDREN WITH TRACHEOSTOMIES IN INTENSIVE CARE!
What are indications for mechanical home ventilation and Intensive Care At Home?