


Podcast: Play in new window | Download
Hi it’s Patrik Hutzel from INTENSIVE CARE AT HOME where we provide tailor made solutions for long-term ventilated Adults & Children with Tracheostomies and where we also provide tailor made solutions for hospitals and Intensive Care Units whilst providing quality services for long-term ventilated patients and medically complex patients at home, including home TPN.
In last week’s blog, I talked about,
You can check out last week’s blog by clicking on the link below this video:
In today’s blog post, I want to answer a question from one of our clients.
What is the Purpose of a Tracheostomy?
Hello and welcome to another Intensive Care at Home and intensivecarehotline.com live stream.
Today’s livestream is about, “What’s the purpose of a tracheostomy?” Before we go into today’s topic, just a few things about me in case you’re wondering what makes me qualified to talk about today’s topic.
Again, my name is Patrik Hutzel, founder of Intensive Care at Home and intensivecarehotline.com. I’m a critical care nurse. I have worked in critical care for over 20 years in three different countries. I have worked as a nurse unit manager for over five years in intensive care. I am the founder and managing director of Intensive Care at Home, where we provide intensive home care for predominantly long-term ventilated adults and children with a tracheostomy. We also provide BIPAP (bilevel positive airway pressure) or CPAP (continuous positive airway pressure), nursing care at home with intensive care and critical care nurses, Home TPN (total parenteral nutrition), Home IV Fluids, Home IV antibiotics, seizure management, and the list goes on.
I’m also the founder and managing director of intensivecarehotline.com. With Intensive Care Hotline, we are providing a consulting and advocacy service for families in intensive care, all around the world. We advocate and help clients or families in intensive care all around the world, and you can find out more at intensivecarehotline.com.
For today, I will talk about today’s topic of course, and then I will also answer questions that have come in during the week. Feel free to please send your questions into the chat pad and I will answer them here.
Without further ado, let’s get into today’s topic, “What’s the purpose of a tracheostomy?” Well, it depends who you ask, but I’ll give you probably a few variations here. But because we will go down to a degree certain rabbit holes today because it is a complex topic and it’s also not a one size fits all.
So, what’s the purpose of a tracheostomy? It’s a question we get quite frequently, especially with Intensive Care at Home, most of our clients have a tracheostomy. They have a ventilator attached to it. A lot of our clients for Intensive Care Hotline, they come to us saying, “Well, should we give consent to a tracheostomy for my mom, for my dad, for my spouse in ICU?”, and so forth. So, it’s a very important question, what is the purpose?
So, the purpose of a tracheostomy is to create an opening in the neck to access the trachea, also known as the windpipe, and establish an alternative airway. This procedure is typically done in patients who have difficulty breathing or have obstructed airways due to various medical conditions such as severe respiratory issues, trauma, or a need for long-term ventilation support. That sums it up pretty quickly, but that’s just a one paragraph sentence really that doesn’t really talk about the intricacies of what is really the purpose of a tracheostomy.
So, let’s just go into intensive care and have a look at what’s happening in intensive care. Many patients in intensive care are ventilated with a breathing tube or an endotracheal tube. They are in an induced coma very often to be able to tolerate the mechanical ventilation and the breathing tube. If mechanical ventilation and the breathing tube is needed for longer than 10 to 14 days and they can’t be weaned off the ventilator, then the next step often is to suggest a tracheostomy to help with weaning off the ventilator, that is one purpose of a tracheostomy.
Then, the goal is to wean the patient off the ventilator as quickly as possible. Then once someone is weaned off the ventilator but still has a tracheostomy, then the goal is to wean the tracheostomy. There’s plenty of patients out there, adults and kids, that need the tracheostomy initially to wean off ventilation, to buy them time, so to speak, to give them time, and then the purpose is to wean off the tracheostomy or decannulate them.
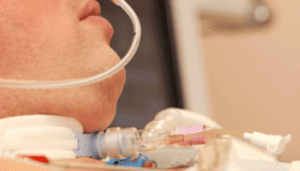
Now, also I want to quickly show everyone what a tracheostomy looks like, that’s what a tracheostomy looks like. It goes into the windpipe and that balloon there will be inflated with some air to keep the tracheostomy in the right place, so it doesn’t fall out. It also provides a seal. I’ll quickly show you what that looks like, inflating the balloon, so you can see what I’m talking about. I’m going to inflate the balloon here so you can actually see what that looks like and you can see the purpose of it. So, I’m going to inject some air now. You can see that balloon going up and that keeps the tracheostomy in. It also makes sure there’s no leak from when there’s ventilator oxygen and air going in because otherwise, it would just blow off in the air. So, that’s the purpose in a short version.
Now, there are patients out there, especially our clientele with Intensive Care at Home that have spinal injuries that require them to have a tracheostomy and a ventilator, 24 hours a day, often for the rest of their lives, if it’s a C1, C2 spinal injury, motor neurone disease, or cerebral palsy as well.
Then in an ideal world, you wean someone off a ventilator, then they’re left with a tracheostomy and then you can remove that tracheostomy as well. Now again, there are exceptions to the rule. Maybe they had a laryngectomy, meaning they had to remove parts of the larynx part of the windpipe, and then that also means that someone needs a tracheostomy for the rest of their life to be able to breathe because air through the nose or through the mouth wouldn’t go into the lungs. So, that could be another scenario.
Furthermore, another scenario could be someone with a stroke for example. They might be able to be weaned off the ventilator and then they can’t swallow. If people can’t swallow, then they also need a tracheostomy and the reason for that is that balloon often needs to be up for someone who can’t swallow, so the saliva that patients can’t swallow doesn’t go into the lungs and cause aspiration pneumonia. So, that’s another scenario for the purpose of a tracheostomy.
So, you can already see, we could go down rabbit holes here in terms of when a tracheostomy and a ventilator is needed. It’s not a one size fits all, even though it often starts on the same sort of notion that a critically ill patient can’t be weaned off the ventilator to begin with. Then once the ventilator has been removed, assuming that is what it’s important, that a tracheostomy can then be removed. If it can’t be removed, it’s often again swallowing, also managing secretions. If someone can’t manage their secretions and can’t protect the airway, they need regular tracheostomy suctioning. That’s another indication or another purpose of a tracheostomy, and that reduces the risk of complication. It reduces the risk for pneumonia, for respiratory events, aspiration, and tracheostomy blockage. If you’re not suctioning frequently, that could cause tracheostomy blockage.
Furthermore, what can happen with a tracheostomy once the ventilator is removed? You can actually use a speaking valve. That means the patient should be able to speak with training initially from a speech therapist, and that means once that’s done, once the speaking valve is on, then a speech therapist can help a patient to start learning to speak again. It’s quite a process for some patients, because basically once the tracheostomy is in, the vocal cords are usually paralyzed, and then you also got to remove the balloon. You’ve got to take the block down, the balloon down, put the speaking valve on, and then hopefully a patient can start to talk again, but that can be also very irritating to begin with. I’ve seen many patients in ICU or at home, when you first want them to talk again and you put the balloon down, it can be very, very irritable for them. It could cause a lot of coughing and splattering and lots of secretions and so forth. So, that is in a nutshell the purpose of a tracheostomy.
But what about long-term? If someone can’t be weaned off the ventilator long-term and has a tracheostomy, it also means that they most likely have or need the tracheostomy for the rest of their lives. It’s a very unfortunate reality in currently. But then another question here is can you have service like Intensive Care at Home if that’s what’s needed? Many patients will stay in intensive care with a tracheostomy or a ventilator because there’s no one for them to go to. Then with our service Intensive Care at Home, we can help you go home. If you’re watching this, and you might be a patient or might be a family member who has a loved one in ICU long-term, you can go home with Intensive Care at Home.
Currently with Intensive Care at Home, we are operating all around Australia. We are sending intensive care nurses and critical care nurses into the home, 24 hours a day, to replicate the ICU bed, the intensive care bed, and offer a genuine alternative, which is a win-win situation. We free up the most sought-after bed in a hospital, which is the ICU bed. We free up nursing staff, we free up medical staff, allied health and so forth by doing so. More importantly, we cut the cost by around 50% of the intensive care bed. Intensive care bed costs around 5 to $6,000 per day.
If the patient is in their long-term and the bed can’t be used for someone that, God forbid, had an accident, or needs surgery, no one’s winning. So by us taking those patients home, it’s a win-win situation, everyone is winning.
The challenge with the tracheostomy is to look after tracheostomy. It’s a highly specialized skill. It’s only intensive care nurses that can look after tracheostomy or anesthetic nurses or ED, emergency nurses. Nobody else really has the skill and if they say they do, they’re just pretending because you can’t just learn the skill to manage a tracheostomy in a crash course or in an e-module online. You need to have hands-on experience for many years before you can confidently say you know how to manage a tracheostomy and a ventilator.
So, it’s a really important skill to have. It’s a very rare skill to have. Not many people really know how to competently manage a tracheostomy, especially when it comes to medical emergencies as well. You need to know what to do when it comes to airway compromise with a tracheostomy. You need to know what to do when a tracheostomy, for example, is blocked. If you don’t know what to do when a tracheostomy is blocked, for example, patients have died and continue to die if they’re not looked after by intensive care nurses or critical care nurses.
Case in point, we have looked after tracheostomy and ventilated clients at home with the tracheostomy, adults and children, that were funded for nursing care only overnight where we had critical care nurses overnight for a night shift. Then during the day, the funding body, in this case, the NDIS here in Australia, was not funding the critical care nurse and the clients, just as we predicted at the time, passed away during the day because the families or support workers, basically non-trained staff, could not manage a medical emergency. Why do you think that patients with a tracheostomy are generally speaking in intensive care and not at home with lay people? That’s why they’re at home.
With our service Intensive Care at Home, we are third party accredited to offer and provide Intensive Care at Home. We are government-accredited to provide that sort of service. We are the only service in Australia, as far as I’m aware, in 2023 that has achieved that level of accreditation. So, we are well-qualified and well-placed to replicate the intensive care a bit in the community, that is our skill.
Currently with Intensive Care at Home, we predominantly operating in Australia. We are going to the U.S. very soon. But if you’re in the U.S., please contact us anyway. Or if you’re in the UK, please contact us. We have helped families in the U.S. and in the U.K. going on to different providers or helping them to look at creative solutions to make sure their loved ones are not stuck in intensive care for the rest of their days. So, contact us one way or another.
If you are an NDIS support coordinator and you’re watching this and you haven’t heard of a tracheostomy before, you don’t know what a tracheostomy is, but you realize your NDIS participant or client has a tracheostomy and you’re potentially giving them the wrong support, now that you know that patients have died or participants have died under the watch of the NDIS, because the NDIS wasn’t funding the right level of support, you should contact us urgently.
So, coming back to the purpose of a tracheostomy, I think it’s also important to know that in most cases, the purpose of a tracheostomy should be short-term measure only. As much as I’m exposed with Intensive Care at Home to long-term tracheostomy, I should also very much make it clear here that the purpose of a tracheostomy can only be ever a short-term device, short-term piece of equipment to help patients to wean off the ventilators as quickly as possible. Once that’s achieved, remove the tracheostomy as quickly as possible, that should always be the goal. In some cases, it can’t be achieved. We all know that here at Intensive Care at Home in particular, but you do know what I’m saying here that it can only ever be a short-term measure.
Also, disclaimer here, this is specifically for our U.S. client based, especially for Intensive Care Hotline. I know that if you’re watching this and you have a loved one in intensive care and the intensive care team wants to do a tracheostomy as quickly as possible, you might be in for something different coming. So, in the U.S. in particular, a tracheostomy is often a vehicle to send patients out of intensive care to LTAC as quickly as possible. Now, I don’t know you watching this video in the U.S. whether you know what an LTAC is. LTAC stands for Long-Term Acute Care facility or Long-Term Acute Care hospital, and it’s not even the better version of a nursing home. Basically, patients from ICU as soon as they have a tracheostomy in the PEG tube, go to LTAC as quickly as possible unless you put a stop to it because that’s a lot of the work we are doing with Intensive Care Hotline.
We put a stop to patients going to LTAC when families hire our service because we know the tools, we know the tricks, we know all the ins and outs to keep patients in the right environment and not let them go to LTAC, which is really unsafe and negligent. So, before you have another thing coming with your loved one, getting a tracheostomy in ICU in the U.S. in particular, and the next thing you know the ICU is trying to push you out to an LTAC. You have to do your research pretty quickly.
So, here’s what you should be doing from my decades of experience. A tracheostomy has its time and its place. I’m not opposed to a tracheostomy. It has its time and its place for the right patient. Again, I’ve made counters of videos and written countless blog posts about this, “When to do a tracheostomy?” That’s not so much our topic today, but a tracheostomy has its time and its place. If it’s used for good, it’s a good thing. But if it’s used for negative things, if it’s used for pushing agendas that are not in the best interest of your loved one, again, you’ve got another thing coming and you’ve got to do your research and you need to know what you’re talking about.
So, here’s what I mean by that. Let’s just say your loved one is in intensive care for 7, 10 days on a ventilator with a breathing tube and they have a good chance to come off the ventilator, but they’re still in an induced coma. They’re bit complacent, a bit lazy. They’re not taking your loved one out of the induced coma, but they’re suggesting a tracheostomy instead. You don’t know any better, you give consent to a tracheostomy and the PEG (Percutaneous Endoscopic Gastrostomy) tube. The next thing you know, your loved one is being shipped out to an LTAC the next day after the tracheostomy and the PEG tube have been done.
We’ve seen this and families have no idea that by the time they’ve given consent to a tracheostomy and the PEG, intensive care team didn’t tell them that the next step is to send their loved ones to LTAC. It’s sort of bait and switch, selling them that the tracheostomy is the best thing since sliced bread. The next thing you know, they’re in LTAC the next day. Families can see pretty quickly that they’ve gone into what’s not even a better version of a nursing home and they’re going from ICU to what’s not even a better version of a nursing home, so very unsafe.
The alternative here in the example that I just gave is always ask the intensive care team, what have they done beyond the shadow of a doubt to wean their loved one off the ventilator and the breathing tube and avoid the tracheostomy? If someone is in an induced coma or in a prolonged induced coma, I argue, intensive care team haven’t done what they could do beyond the shadow of a doubt to wean their loved one off the ventilator.
I’ve written an article about, “How to wean a critically ill patient off the ventilator and the breathing tube?” You should be checking out that article or watching the video for your own guidance to avoid a tracheostomy in many cases. So, be on high alert especially if you’re watching this and you are in the U.S. when it comes to ICU and then going into LTAC. Do not give consent to a PEG tube either. Do not give consent to a PEG tube, no need for it. A nasogastric tube will do. Again, I’ve made videos about this before.
Also, on the other hand, if your loved one has been in intensive care for four weeks, for example, and is still on a breathing tube on a ventilator, can’t be weaned off, then a tracheostomy is probably the right thing to do. But you have to wonder then why did the intensive care team not tell you about doing a tracheostomy after day 10 to 14? I’ve seen both extremes. I’ve seen both extremes. So, you have to do your own research. You have to be on high alert when it comes to these very important issues. You can’t just fly blind. You have to understand the purpose of a tracheostomy.
Once you understand the purpose of a tracheostomy, it’s much more difficult for you to be misled by the intensive care team. It’s much easier for you to then push towards the right decisions, push towards the right treatment options for your loved one in intensive care.
Helene, nice to see you. You are saying this is what happened to your mom. Can you be more specific? What happened to your mom? Tracheostomy too early or tracheostomy too late?
So, this is what I mean by the purpose of a tracheostomy. It’s not a one size fits all. It all depends. As much as you might think, “Oh, a tracheostomy is the only way forward here.” What you want to find out one way or another is, has the intensive care team potentially messed up before you did the tracheostomy? Have they potentially messed up? Could the tracheostomy have been avoided? Could it have been done much earlier?
The bottom line is one of the take takeaway messages here today needs to be a tracheostomy cannot be safe outside of intensive care or on a respiratory ward or with Intensive Care at Home. Everything else is futile and has cost people’s lives. So, very important that you understand the correct steps when it comes to a tracheostomy, when it should be done? Is it the right thing to do? Are there alternatives? Can it be avoided?
Helene, I still don’t know what you mean with, this is what happened to your mom with a tracheostomy. I don’t know what you mean. Maybe if you can elaborate, that would be good.
Now, let’s also look at some questions that came in during the week. So, let’s look at some questions that came in during the week so that we can answer some of them. I’ve just got to get to my emails, and I do need to check what’s come in this week, so much that came in. I just need to quickly send a very quick text to a client actually, to an Intensive Care Hotline client. So, let’s look at questions from this week.
Helene, you’re mentioning now, “Tracheostomy was forced and lied to cover up iatrogenic malfeasance injuries and drug induced respiratory failure.” Yeah, no surprises there. That’s what I meant earlier, Helene, when I said if you keep someone in an induced coma for too long, a tracheostomy is almost inevitable. Whereas if you don’t sedate people in the first place and or keep them lightly sedated, it’s so much easier to wean them off the ventilator and avoid a tracheostomy, do the right things, and get them to extubation as quickly as possible. That should always be the goal.
Again, I do want to reiterate that. The goal for someone on a ventilator is to wean them off the ventilator and the breathing tube as quickly as possible. If that can’t be achieved, do a tracheostomy once again with a goal to wean someone off a ventilator as quickly as possible and then wean the tracheostomy and decannulate them. That should always be the goal. None of it should be a long-term solution with the exception of someone with a spinal injury, motor neurone disease, type 1, type 2 longstanding respiratory failure. Sure, there’s the exception to the rule, but they are exceptions.
As much as we are exposed to these exceptions with Intensive Care at Home, we are talking about a small number of people here, a large number of people in intensive care that might have tracheostomies, but again, always try to wean as quickly as possible, one way or another.
So now, let’s look at a question that came in this week. Charles says, “My sister has been in ICU for three weeks, treated for almost every organ, dialysis, lungs, heart, et cetera. She suffered a stroke and massive cardiac arrest while in ICU and after the induced coma was removed, she couldn’t wake up. They performed a brain scan and found that her brain is swelling. Now, they have informed the family that medically, there’s nothing they can do. They took her off everything except the ventilator. How long will she still be alive and does the ventilator do any good?” Great question, Charles. Well, it really depends how severely damaged her heart, lungs, et cetera are. She sounds like she’s medically stable now. The brain is swelling. The brain swelling will probably come down eventually. It sounds to me like from the stroke, she might have a hypoxic brain injury or an anoxic brain injury or with a cardiac arrest as well.
Now, so the question here is this, Charles, you’re saying she’s still on the ventilator. Is she on a ventilator with a breathing tube or does she need a tracheostomy now? If she’s been in ICU for three weeks and she’s still on the ventilator, she can’t come off the ventilator, ties right in with our topic today. Then the purpose should be to do a tracheostomy assuming you want to prolong her life and you want to give her every chance that she may recover, even if she can’t fully recover, that is up to you and your family what you would perceive as the best option here.
Let’s just say she can’t come off the ventilator and she can’t come off the tracheostomy or even if she can come off the ventilator, but she can’t be off the tracheostomy, then definitely Intensive Care at Home is an option for you, for your family to take your sister home, including end of life care, if that’s what it might be, if it’s end of life care. How long can the ventilator keep her alive? Potentially for a long time, especially if there’s good care associated with it like we do with Intensive Care at Home. She can be alive for a long time to come, but you got to be clear about the goals of care for your sister.
If they’re saying they have informed you that medically there’s nothing they can do, well, question here, does she need to go to neurology rehab? That’s the question here. Is that possible? If she can’t go to neurology rehab for whatever reason, can she go home once again with Intensive Care at Home for either ongoing recovery? If that’s possible, ongoing rehabilitation at home, or is it potentially end of life care/palliative care at home? Those are the questions.
We’ve asked today, what is the purpose of a tracheostomy? You could also argue that the purpose of a tracheostomy is sometimes to facilitate end of life care, facilitating end of life care including facilitating end of life care at home. We’ve done that too with Intensive Care at Home. If that’s people’s wishes to have end of life care at home, we can facilitate that with Intensive Care at Home. So, go to intensivecareathome.com and have a look there and contact us on one of the numbers on the top of our website or send us an email to [email protected].
Now, Helene, you are saying here, “Iatrogenic induced hypoxic encephalopathy, permanent brain damage. They refuse to decannulate her and were discharged to LTAC.” Yeah, sure. Typically, for many clients in the U.S., that this is unfortunately what’s happening. Your late mother’s iatrogenic malfeasance tortured, and injuries were due to exploiting her for false claims for fraud. Helene, I am just absolutely mortified by your and your mom’s situation when she went into ICU and into LTAC. I know there have been some terrible things happening to your mom.
Let’s look at another question that’s coming this week from Betty. Betty says, “I just bet that the patient’s insurance is at the root of the decision making in ICU. The patient needs to have continued ICU care, as long as the patient wants it. The patient wants to live, plain and simple. My mother is still alive and in a sound mind, at least it sounds as if she is, and then is the end of it until she changes her mind. God bless and keep safe, all the patients in ICU, and those that are not but need to be until they can arrive at a place of good health.” Yes, absolutely. Thank you for that comment, Betty.
I agree with you that many of the decisions based in ICU are based on insurance, based on bed status, bed availability, staff availability, how much control that intensive care teams want to give families. That’s also something we’ve changed with Intensive Care at Home. We are now giving patients, families, as well as ICUs options to get patients home. We’ve also done things like we know of some patients that have been at home and had lots of hospital and ICU readmissions because they didn’t have the ICU nurse at home, the critical care nurse at home. Therefore, they ended up going back to ICU and we put a stop to that.
Another thing we are doing at the moment with Intensive Care at Home, we started basically being an ED, emergency department or emergency room bypass service in Sydney for the Sydney Western Local Health District where we help them keep their EDs empty, where we go to people’s homes and basically provide an ED nursing service to avoid ED readmission. So, that’s another skill we are bringing to the table, critical care nurses in the home.
Another comment from Carly this week that came in says, “What was happening during the COVID lockdowns inside the hospitals when politicians made the law stating no visitors unless end of life for immediate family?” Well, that was a terrible time. I don’t think that anyone would remember COVID and COVID lockdowns with much pleasure here. Whether you buy into the COVID narrative or not, I do believe that hospitals should not have locked out family members, especially for dying patients. I do believe that families are traumatized now if they had a loved one dying in intensive care that they couldn’t visit in person. I do believe that many families are traumatized. We are hearing their stories from them now, saying, “My love one was in ICU during COVID. I couldn’t visit them and they were dying.” It sounds absolutely horrific.
Next question from Rebecca. Rebecca says, “My father-in-law is in ICU right now. He had a quadruple bypass yesterday morning and either in surgery or in recovery had a stroke. As of now, he has not woken up and is not responding to commands. He’s off all sedation, and they even used Narcan, which didn’t work. They have confirmed that he did have a stroke through the CT scan of the brain. Now, his kidneys are declining slightly, but that could be from dehydration and being on the pump for so long. It’s killing us not knowing but what can you do but wait and hope for the best.” Thank you, Rebecca, for writing in and asking that question. One day in ICU after cardiac surgery that didn’t go well is probably too early to jump to any conclusions. Yes, he’s had a stroke, which is no good, but it depends on the severity of the stroke, whether he can recover or not.
So, here’s what’s important. When someone had bypass surgery, they’ve been in an induced coma for many hours. If he’s had a quadruple bypass, it would’ve been a few hours in surgery. He would’ve been on the bypass machine, on the ECMO (Extracorporeal membrane oxygenation) machine. Yes, he would’ve potentially been dehydrated through that and that might have caused the kidney failure. He might have also been hypotensive, low blood pressure during surgery, and that might have contributed to kidney failure.
But one day in ICU, even though many things have gone wrong, doesn’t mean you should be giving up. It’s very early days. Patients after cardiac surgery sometimes don’t wake up even if there’s no brain damage because they have been in an induced coma for prolonged periods. So, don’t jump to conclusions just as yet. Give this some time, give it at least a few days, potentially up to a week, and then see where you’re going from there.
If the Narcan didn’t work, yes, that is a sign that he might have got a severe stroke. That is definitely a sign for that because Narcan is basically an antidote to morphine or opiates. So therefore, if the Narcan didn’t work, yes, there’s a high chance he does have some severe stroke or brain damage, but again, you got to give this some time. Some patients with a stroke do recover.
I hope that next month I can actually bring on my friend Bill who is actually a stroke survivor and talk about his journey. I’m planning to do that podcast here next month. Well, I’ll talk to my friend Bill. He will have a lot of insights about how to survive a stroke and how to recover from it.
Also, when patients are in intensive care, like in your father-in-law situation here, Rebecca, it’s not unusual that things like that happen in intensive care. That’s why patients go into intensive care in the first place to deal with these challenges. So, it’s very early days, don’t give up. Let’s see whether the kidneys recover. He could go on dialysis. He could have a tracheostomy if he’s not waking up again, which ties right in with our topic today. If he doesn’t wake up and you want to give him every chance, he might need a tracheostomy and that gives him more time to recover, could also give him the time to go home, continue with rehabilitation at home if it’s possible at all. If it’s not possible, can he have end-of-life care at home, spend more time with the family if he has a tracheostomy, again, with our service Intensive Care at Home.
Helene, you are saying, “I was traumatized for what I horrifically witnessed. It was modified that mom’s ICU providers tried to make me their scapegoat.” Well, Helene, I really hope you’ve got some closure around this and I really hope you’ve got some lawyers on this case. I don’t know. I don’t want to be jumping to conclusions here, but I know you’ve talked about this to me before, either on this, on the YouTube live, or on a phone call. I really hope you can get some closure in regards to this issue, and I really hope you can take the people that are responsible for this and hold them accountable. I really hope you can do that.
Let’s go to another question quickly and this is from Betty. This is another comment that Betty sent in this week. Betty says,
“As a retired critical care nurse for over 35 years, I am continually astounded by the families that have a loved one in ICU or NICU and blindly accept whatever a doctor says or a team says without doing any research on them, their education and research on the loved one’s illness before giving consent to care.
I have practiced in the United States all of my career and have seen our medical care plummet from the best to the worst. It has become all about money. The patient is no longer the first and foremost concerned. It is about your insurance coverage, your age, your demographics, and your ability to pay.
All healthcare is governed by big pharma and insurance companies that control the individual caregiver and especially the doctor. I have always believed that a patient’s care is directly dependent on the caregivers’ personal sense of morality and ethics. If they have them, they will give you the care, they would give their own family. If it’s merely a job and they’re so burned out that they don’t care, the patient is hopeless to get any good quality care.
I refuse to put my patient last and ultimately quit nursing because of it. I now believe Singapore and then the NHS gives the best care on the planet right now, but it’s ultimately the responsibility of the family to see that their loved one gets the right care. That takes work and sadly, many do not want to invest the time.”
Well, I can pretty much concur with all of what Betty says here. The only thing that I don’t concur is once, I can’t comment about Singapore, I can comment about the NHS. I do argue that the NHS in the U.K. is actually the worst at system in English-speaking countries. I do believe that the U.S. is actually better than the NHS. It’s not perfect by any means, but the NHS is, I argue, the worst system in English-speaking countries. I believe there is euthanasia happening left, right, and center.
I believe that has been evidenced by some public cases lately or in the last few years. I only mentioned Charlie Gard, Alfie Evans, and Archie Battersbee are just three prominent cases where I argue the NHS did not act in their best interest, did not let them go overseas for treatment. Those children, keep in mind, they were children died in the hand of what I perceive as a communist NHS healthcare system. So, keep that in mind.
But other than that, I concur with what you’re saying there, Betty, when I work in ICU, I also realized I can no longer do this because people have lost all morals. They have lost all ethics for whatever reason. Some of it is certainly money, but we can’t let our medical system play God and have some element of population control if you want.
Helene, you’re saying that you are planning to do that, to take someone to account, get a bunch of lawyers or whatever your next steps are. You’re also saying, “Uninformed consents and lied to by ICU providers.” Yeah, that’s extremely disappointing, Helene, and I really hope that the right people will be held accountable for what’s happened to your mom.
So, the next question comes from Hannah. Hannah says, “Any tips for someone with intellectual disabilities who has been on a ventilator for the past 16 days? Looking into tracheostomy now, but currently needs sedation and restraints to prevent from pulling out the breathing tube. How can he manage recovery with tracheostomy if he needs restraints?” Well, this is a great question and it’s a question that again ties in with today’s topic, what is the purpose of a tracheostomy?
Well, I argue if he’s that combative, it sounds to me like there’s a level of combativeness. If he’s that combative, I argue, depending on what the ventilator settings are, he might be able to have the breathing tube removed and not need a tracheostomy because it is combative. That means he must be strong. If he’s strong, he can breathe. So, it’s also a good sign if he can pull out the breathing tube. Now, I’m not advocating for him to pull out the breathing tube, not at all. But what I am saying is it would be good. It’s a good sign that he can pull out the breathing tube because it means he’s strong.
So, here is my tip. Let’s take sedation is off and he’s still agitated, but he’s on minimal ventilator support. Can someone mainly family help him? Can they talk him through it? Can they morally support him? Can they hold his hand? Can they talk him through it? Can the doctors and nurses talk him through it?
So, in this situation, it’s 16 days. The time has sort of passed for a tracheostomy, it’s sort of passed. He should have had a tracheostomy by now. So, why have they waited for 16 days? Why have they waited for 16 days if they’re preventing him from pulling out the breathing tube by using restraints, once again, I do believe that he’s strong. That’s a good sign.
Let’s just say he doesn’t need a tracheostomy. Let’s just take the worst-case scenario. You should be able to take him off sedation because the tracheostomy is much easier to tolerate compared to a breathing tube. So much easier to tolerate, much, much easier. So therefore, the need for sedation should have been diminished and therefore he shouldn’t need restraints. Most people try and pull out the breathing tube because it’s extremely uncomfortable. Not many people try to pull out the tracheostomy because it’s much more comfortable. So therefore, the need for sedation should be gone. Again, his strength would improve by not using any sedation, and then hopefully he can just get the tracheostomy removed as well, assuming he’s on minimal ventilator settings. But if he’s that strong, his ventilator settings might be minimal as well. I hope that helps, Hannah.
Let’s move along to the next question from Susan. Susan says, “My father has been in ICU since January 22 with multiple factors weighing against him. He’s the highest decorated firefighter in Dallas, Texas, and has been fighting for his life. This all started 20 months ago with an abscess tooth that has now led to multiple problems. I would love to talk to you, Patrik. If possible, here’s my email and my cell phone. I’m helping my mother with her bills as she has been overdrawn all year, so I cannot afford the price on your side. I was wondering if Patrik could review my father’s case as a charity situation. I’m having to try and pay their utility bills via GoFundMe that is not gaining much traction. My father has a YouTube channel I made, obviously keep names confidentially here. Thank you if you read this for a reply, from Susan.” Susan, that’s very sad to hear.
Unfortunately, I do not do any charity work. I do have a team in the background working with me. They all need to be paid. So, we do need to earn a living doing what we’re doing here. But I’m confidently charging what I’m charging because we’re getting outcomes for families. We’re getting real results for families.
I’ll give you on this point, on this notion. Last night, I had an inquiry, or yesterday afternoon I had an inquiry, basically telling me, “Hey, we have family member in intensive care. They’re telling us she’s brain dead and tomorrow morning at 10 o’clock they want to remove life support and let her die.” I said, “Okay, tell me more.” So, the client booked a couple of hours with me yesterday, and within no time really, we were able to turn this situation around.
Now, if someone is declared brain dead in most cases, whether it’s in the United States, in Australia, and the U.K., if someone has been declared brain dead, they are most of the time also legally dead. But I question that because I’ve seen so many times where intensive care teams say, “Oh, your loved one is brain dead.” They have not done the brain death testing, and they often sometimes mislead families and say someone is brain dead, when in reality, they have brain damage and there’s a big difference there. Big difference between someone being brain dead and being brain damaged.
So, what we did then is I wrote a letter to the hospital CEO and within a few hours, bear in mind, this was on a Saturday night, within a few hours, the hospital CEO comes back and says, “Yep, we won’t remove life support tomorrow morning.” I know the ins and outs of ICUs. I know the ins and outs of hospitals. I know that patient and family rights. Now, I didn’t know whether the patient was legally dead or not. I didn’t know that, but I assume the patient is not legally dead because otherwise they would be well within their rights to stop life support. But given that they didn’t do that well, she mustn’t be legally dead and brain dead.
So, please keep in mind if you want free advice from me, I encourage you to watch my videos. Come on the YouTube live shows if you wanted free advice. There are so many videos out there and blog posts that you can just watch and you will get all the advice you need. But if you want to get the shortcut and not watch all the videos, then I do charge a fee and I do it with a very good conscience.
Next from Beth. Beth says, “Thank you so much for sharing all your videos and blog posts. My mother is in ICU too since the 5th of June to present. Her husband wanted to take her off this Tuesday. What do you think of that? Her brain was damaged due to sedative propofol being administered.” Well, I’m not sure whether brain would be damaged just by some propofol. I’m not sure about that, but there might be an exception to the rule.
Should you take your family member off life support? Well, it all comes down to whether it’s a real or a perceived end of life situation. Well, if you need to take someone off life support, I argue it’s a perceived end of life situation. So, the difference between a real and of perceived end of life situation, quite frankly, is that a real end of life situation means that no amount of life support, no treatment, no surgery, no medication, or nothing will save your love one’s life, full stop. A perceived end of life situation is can you keep someone alive? If you can, and you’re actively withdrawing life support, that in my mind is a perceived end of life situation. That means you can keep someone alive. So, it comes back to that.
It also comes back to the goals of care. Maybe your mother has an advanced care directive saying, “Well, I don’t want to live in ICU. I don’t want all resources to be made available to me. I don’t want all treatment options to be made available to me.” Maybe that is what your mother said, and if that’s what she said, then maybe that’s where it needs to go to. But you need to find out what your mother would want if she could make her own decisions in a situation like that and go from there.
Remember this, there’s no return from death as far as we know. Meaning, if your mom has passed away, you might have regrets. Another tip here is to make decisions that you don’t regret in 12 months’ time. Make decisions today that you don’t regret in 12 months’ time. Now, if you pull the plug today, excuse my language here, you might have regrets and you might not be able to sleep at night knowing that you haven’t done everything could drop you off sleep, could drop you off peace of mind, could drop you off a lot of things. More importantly, it’ll drop you off your mom by the sounds of things. So, think that through very carefully. We can give you a second opinion. Reach out to us. That was Beth’s question and then we will go to that question next week.
So, I hope that was a good session today. Any more questions around tracheostomy, just post it beyond this video. I want to thank you for coming onto the call or to the show in real time, live, and posting your questions here, but also welcome you to watch this afterwards, of course.
If you have any questions, type them into the chat pad or contact us at intensivecareathome.com. Call us on one of the numbers on the top of the website, especially if you have a loved one in intensive care or if you’re a patient yourself and you want to go home, then I’m assuming you’re stuck in ICU long-term, or you might be in a rehab facility with a ventilator and the tracheostomy. Anything related to ventilation, tracheostomy, BIPAP, CPAP ventilation, VPAP ventilation, home TPN, IV fluids, IV antibiotics, IV electrolytes, come to us at intensivecareathome.com.
Currently, we are operating all around Australia and we employ critical care registered nurses to go into the home. We are NDIS (National Disability Insurance Scheme), TAC (Transport Accident Commission), DVA (Department of Veteran Affairs), iCare, QIIS approved service provider. We are also currently working with the Western Sydney Local Health District to prevent ED readmissions.
If you’re an NDIS support coordinator and you’re looking for help with nursing care for your NDIS participant with tracheostomy ventilation, everything that I mentioned just now, please contact us as well. Please don’t be shy because we are learning that a lot of NDIS support coordinators don’t even know that nursing care through the NDIS is an option. We would really welcome to talk to you. We can show you the ins and outs, how to make that happen. Contact us at intensivecareathome.com. Call us on one of the numbers on the top of our website or send us an email to [email protected].
If you have a loved one in intensive care and you need consulting and advocacy, go to intensivecarehotline.com. Call us there on one of the numbers on the top of our website or email us to [email protected].
We also offer nursing assessments for the NDIS and for any other funding bodies. We also offer medical record reviews for intensive care patients even in real time.
If you are a critical care nurse and you’re looking for a job in Australia, please contact us as well. Our main jobs at the moment are Brisbane, Sydney, and Melbourne, or Country Victoria and Country New South Wales as well. Please contact us for that. Ideally, you have a minimum of two years critical care nursing experience before you work with us and be adaptable, be flexible, have an open mind, that would be very important.
If you are an intensive care specialist, please contact us as well. If you need help with managing your ICU beds or if your hospital executive, please contact us as well.
Subscribe to my YouTube channel for regular updates for families in intensive care, click the like button, click the notification bell, share the video with your friends and families, and comment below what you want to see next, or what questions and insights you have from this video.
Thank you so much for watching.
This is Patrik Hutzel from intensivecathome.com and I will talk to you in a few days.
I’ll also do another YouTube live next Sunday, 10:30 AM Sydney, Melbourne time, which is 8:30 PM, Saturday evening, Eastern Standard Time in the U.S., 5:30 PM on a Saturday, Pacific time.
Take care and have a great week.
Now, if you have a loved one in intensive care and you want to go home with our service Intensive Care at Home and if you want to find out how to get funding for our service and how it all works, please contact us on one of the numbers on the top of our website, or send me an email to [email protected]. That’s Patrik, just with a K at the end.
Please also have a look at our case studies because there we highlight more about what we can do for clients, how clients can live at home with ventilation and tracheostomies and you can look at our case studies as well at our service section.
Intensive care at home Case studies
And if you are at home already and you need support for your critically ill loved one at home, and you have insufficient support or insufficient funding, please contact us as well. We can help you with all of that.
And if you are an intensive care nurse or a pediatric intensive care nurse with a minimum of two years, ICU or pediatric ICU experience, and you ideally have a critical care certificate, please contact us as well. Check out our career section on our website. We are currently hiring ICU and pediatric ICU nurses for clients in the Melbourne metropolitan area, Northern suburbs, Sunbury, Bendigo, Mornington Peninsula, Bittern, Patterson Lakes, Frankston area, South Gippsland, Drouin, Warragul, Trida, Trafalgar and Moe as well as Wollongong in New South Wales.
www.intensivecareathome.com/careers
So we are also an NDIS, TAC (Victoria) and DVA (Department of Veteran Affairs) approved community service provider in Australia. Also have a look at our range of full service provisions.
Thank you for watching this video and thank you for tuning into this week’s blog.
This is Patrik from Intensive Care at Home, and I’ll see you again next week in another update.
RELATED LINKS:
 How we can help you
3 quick steps on how to position and prepare yourself well mentally, whilst your loved one is critically ill in Intensive Care
Calls for changes in end of life care!
PODCAST WITH ANTHONY BARTL, A YOUNG MAN WHO IS VENTILATED WITH TRACHEOSTOMY AT HOME! LISTEN TO ANTHONY’S INSPIRATIONAL STORY!
Parents of 2 year-old on life support fight to bring her home!
How we can help you
3 quick steps on how to position and prepare yourself well mentally, whilst your loved one is critically ill in Intensive Care
Calls for changes in end of life care!
PODCAST WITH ANTHONY BARTL, A YOUNG MAN WHO IS VENTILATED WITH TRACHEOSTOMY AT HOME! LISTEN TO ANTHONY’S INSPIRATIONAL STORY!
Parents of 2 year-old on life support fight to bring her home!